
Cranial cruciate ligament (CCL) rupture is the most common cause of lameness in dogs requiring surgery. It leads to knee instability, pain, and progressive joint damage if left untreated.
The cranial cruciate ligament (CCL) is located inside the knee (stifle), and its main role is to prevent the shin bone (tibia) from sliding forward relative to the thigh bone (femur). In dogs, it plays an even more important role than the ACL does in people — without it, the joint will always become misaligned during weight-bearing.
Unlike people, dogs usually don’t tear their CCL from a single injury. Instead, the ligament gradually degenerates over time. It can look like a sudden injury, but the damage has usually been building quietly. The cause isn’t fully understood — it may relate to how the joint is loaded (biomechanics) or something within the ligament itself (biology).
Once the ligament weakens or tears, the joint becomes unstable, leading to inflammation, pain, and eventually arthritis. This often causes ongoing lameness if not treated. CCL disease can affect dogs of all sizes, ages, and activity levels.

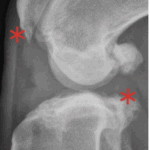
With time, arthritis sets in. Arthritic change includes new bone formation around the joint, called osteophytosis (asterisks).
Dogs with CCL rupture almost always show lameness in the affected hind limb. You might also notice your dog sitting with the leg out to the side. Sometimes both hind limbs are affected, which can cause significant difficulty rising or walking. Some dogs develop a clicking or popping sound from the knee when walking — a sign of possible meniscal damage, a common secondary injury.
Symptoms can appear suddenly or develop slowly as the ligament weakens. A traumatic event is not typically observed, though it’s common for owners to think one caused it.
A veterinarian should perform a careful orthopedic examination and x-rays (radiographs) of the stifle. Features such as pain, range of motion, and muscle mass are assessed. Your vet might recommend a sedated exam to better evaluate joint laxity. Occasionally, a joint tap (sampling joint fluid) may be needed to rule out other conditions.
Orthopedic exams can be tricky, which is why it’s best to have someone skilled and experienced evaluate your dog.

Some dogs with CCL disease can be managed without surgery — especially smaller or less active dogs. Treatment usually includes
rest, anti-inflammatory medication, physical therapy, and weight management. Over time, some dogs develop scar tissue that provides partial stability. However, persistent or worsening lameness is common as arthritis develops.
When both knees are affected, it can severely impact mobility and quality of life, and successful medical management becomes less likely.
Most dogs with a CCL rupture benefit greatly from surgery. Several techniques restore stability to the knee, including:
While techniques differ, all aim to restore stability and reduce arthritis progression. The
Tibial Plateau Leveling Osteotomy (TPLO) is considered the gold standard, offering the most consistent return to near-normal function with a low complication rate — particularly when performed by experienced surgeons.
Surgery typically includes arthroscopic joint inspection to confirm the diagnosis and assess the meniscus, a shock-absorbing cartilage structure. If torn, it’s addressed during the same procedure to help prevent ongoing pain or lameness.

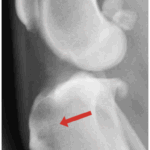
Patellar luxation — when the kneecap slips out of place — is one of the most common orthopedic conditions in dogs. In some pets it causes pain and lameness, while in others it causes no issues at all.
Patellar luxation occurs when the kneecap (patella) slips out of its normal groove at the end of the femur. The patella is a small bone embedded at the end of the quadriceps muscle. This condition is usually developmental, caused by abnormal alignment of the quadriceps and the underlying femur.
The patella most often luxates toward the inside of the leg (medially). Severity can vary widely — from mild cases that cause no pain to advanced deformities that significantly affect movement.
Patellar luxation is especially common in small dogs, but it can also occur in large breeds, where it tends to cause more obvious lameness. Cats can also be affected, and when they are, it’s often more problematic.

The knee on the left has a patellar luxation. The knee on the right is normal.
Many — if not most — dogs with patellar luxation show no obvious symptoms and may live comfortably without intervention. When signs do occur, they often include skipping, hopping, or hind limb lameness.
In more severe cases, dogs can have visibly deformed hind limbs, often with a crouched or hunched posture. Dogs are most often symptomatic when they are young (4 months to 2 years old), although signs can occasionally appear later in life.
A thorough orthopedic examination is important to assess the direction and severity of the luxation, evaluate limb alignment, and look for signs of deformity. Concurrent issues such as cranial cruciate ligament rupture are possible and can also be detected on a good exam.
Radiographs (x-rays) may be recommended, especially if your dog is symptomatic. They are used to evaluate bone alignment and assist with surgical planning. In high-grade or complex cases, CT imaging can be especially helpful for detailed assessment of the bones and joints.

A dog with severe patellar luxation and concurrent limb deformities.
If your pet isn’t showing symptoms, surgical intervention is not usually indicated. Surgical correction is generally recommended for dogs with persistent symptoms. The goal of surgery is to restore proper alignment and tracking of the patella.
Common procedures include:
In more complex cases, corrective bone cuts (osteotomies) of the femur may be necessary to address underlying limb deformities.
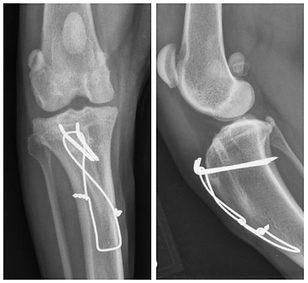
Pins and wires are used to stabilize a tibial tuberosity transposition, the most common surgery for patellar luxation.
If your dog is not experiencing any symptoms, there’s a good chance that the condition will be well tolerated in the long term. Some dogs may become lame in the future if the luxation worsens or if a cruciate ligament tear develops. For dogs undergoing routine surgery, with proper case selection and follow-up care, normal or near-normal limb use is expected. Severe cases, however, may have a higher risk of recurrence or revision surgery.
The menisci are cartilage-like structures in the knee that help distribute weight evenly across the joint. In dogs, meniscal injury most often occurs along with a torn cranial cruciate ligament (CCL).
The menisci are two crescent-shaped, cartilage-like structures located between the femur and tibia within the knee joint. They help cushion impact, stabilize the joint, and distribute weight evenly across the cartilage.
Menisci are commonly torn or crushed when the joint is unstable due to cranial cruciate ligament (CCL) rupture. Meniscal tears typically cause persistent knee pain. Loss of meniscal function can lead to increased pressure on the underlying cartilage, which contributes to the development of osteoarthritis. Because of its firm attachment within the joint, the medial meniscus is more vulnerable to injury when the knee becomes unstable.
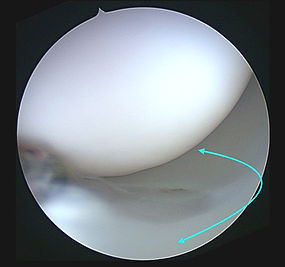
Arthroscopic image of a normal meniscus. The meniscus is crescent-shaped (arrow) and sits between the cartilage surfaces.
Meniscal tears usually occur along with a torn CCL, which already causes lameness. A damaged meniscus can make that lameness worse or more persistent. In some cases, a clicking or popping sound or sensation may be noticed during movement.
Diagnosing a meniscal tear can be challenging. During a physical exam, a clicking sensation in the stifle is strongly suggestive, but not always present. X-rays do not show meniscal damage, though they are often used as part of a full assessment for CCL rupture.
Advanced imaging such as MRI or CT can detect meniscal tears, but these options are often expensive and not commonly used in routine cases. In most dogs, the meniscus is evaluated directly during surgery for CCL injury, either through an open approach (arthrotomy) or a minimally invasive technique (arthroscopy).
Meniscal assessment and treatment are almost always done at the time of surgery for CCL rupture, using either an open approach (arthrotomy) or arthroscopy. Arthroscopy offers better visualization and is much less invasive.
If a tear is found, management depends on its appearance and location. Minor changes are often left alone, while larger or unstable tears are usually trimmed or removed to relieve pain and prevent further joint damage.
The question of what to do with a meniscus that appears intact remains debated. Some surgeons perform a meniscal release to reduce the risk of future tearing, especially in unstable knees. This involves cutting the meniscus attachment to allow freer movement, though it sacrifices normal function and may increase arthritis risk. Many now prefer to preserve the meniscus when it looks healthy, provided the joint is stabilized properly to protect it long term.
Trauma to the stifle in dogs is often complex, as it can involve ligament injury, meniscal tears, or fractures. Proper diagnosis can be challenging, and surgery is usually indicated.
Stifle trauma in dogs is not common, but it’s also not rare. The joint is complex, containing multiple joint surfaces, several important ligaments, and two menisci that act as cushions. Injuries often involve more than one structure.
Ligament damage does not always result from a major collision — it can occur if the leg becomes trapped, during a bad fall, or from a sudden twisting motion.
Fractures inside the joint (intra-articular fractures) are less common but very serious, as they affect the bone surfaces that bear weight. These injuries usually result from high-impact accidents such as being struck by a vehicle.

Complete stifle dislocation, also known as a ‘deranged stifle.’
Symptoms of stifle trauma often include severe lameness, visible swelling, or abnormal joint position. The leg may be held awkwardly and painful to touch. In some cases, the leg may appear normal from the outside, even when significant internal injury is present.
These injuries typically do not heal on their own and require prompt veterinary attention.
Testing for stifle trauma begins with a careful physical exam, as ligament injuries may not be immediately obvious and can sometimes be missed, even by experienced veterinarians. X-rays may reveal fractures but can appear relatively normal when only ligaments are torn.
To evaluate ligament integrity, the veterinarian will often perform stress tests — gently but firmly moving the joint in specific ways to see if it is looser or moves abnormally compared to the other leg. This can reveal hidden instability that is not visible on X-rays.
In more complex or uncertain cases, advanced imaging (CT or MRI) may be necessary to obtain a complete picture of the injury.
Major injuries to the stifle’s key structures almost always require surgery. Depending on the nature of the damage, various reconstruction techniques may be used. Postoperative immobilization with a splint or external frame is often necessary to protect the repair during recovery.
Prompt surgical intervention is critical to restore stability, reduce pain, and prevent further damage. Successful outcomes depend on the experience and skill of a surgeon with detailed knowledge of knee mechanics and anatomy.

Complex stifle trauma repair.
Osteoarthritis is an extremely common problem in both dogs and cats. In some animals, it is well tolerated and causes minimal issues, while in others it can be debilitating. Prevention and treatment recommendations are highly individualized.
Osteoarthritis — also known as degenerative joint disease, arthritis, or osteoarthrosis — is characterized by thinning and wearing of cartilage. It also affects other joint tissues including bone, ligaments, the joint capsule, and surrounding muscles. As the joint degenerates, the underlying bone can become exposed and both soft and hard tissues may thicken. The result is a joint that cannot glide smoothly through a full range of motion.
In dogs, osteoarthritis is usually secondary — meaning it develops as a consequence of another joint problem such as ligament injury, fracture, or developmental disorders like elbow or hip dysplasia. Because secondary OA is so common, identifying and addressing the underlying problem is critical for developing the best treatment strategy.
Classic symptoms of osteoarthritis include:
In cats, signs are often more subtle — such as reduced movement around the home, avoiding touch, or grooming less frequently. Importantly, many animals with osteoarthritis show no obvious symptoms at all.
A careful orthopedic examination is crucial. Affected joints may show thickening, reduced range of motion, pain, or crepitus (a crunching sensation). Multiple joints may be involved, so a thorough exam is essential.
It’s also important to determine any underlying cause. For example, instability in an arthritic stifle may indicate secondary arthritis from a cranial cruciate ligament rupture.
Radiographs (X-rays) are very important for confirming osteoarthritis, identifying the cause, and gauging severity. In some cases, advanced imaging such as CT or MRI can reveal more detail about bone and soft tissue changes. Arthroscopy allows direct visualization of the joint interior and can be used both for diagnosis and treatment of certain causes of secondary OA.
The primary goals are to reduce pain, improve movement, and slow further damage. Osteoarthritis is often managed medically through anti-inflammatory medications, weight control, joint supplements, and physical therapy. Many pets remain comfortable for years with these measures alone.
Surgical options may be recommended for a variety of reasons:
The best approach depends on the joint involved, the severity of disease, your pet’s overall health, and activity level.
Most dogs can enjoy many years of good quality life with the right management plan. The course of the disease varies — some dogs remain asymptomatic for life, while others develop more significant mobility issues over time.
Early diagnosis and proactive care — including weight control, tailored exercise, pain management, and, when appropriate, surgical intervention — can slow progression and greatly improve comfort and mobility.